Designing Attenly — A Child-Centric ADHD Screening App
A collaborative screening tool for parents and teachers to enable early recognition of ADHD symptoms in children aged 6-12, supporting timely professional intervention.

ADHD often goes unidentified in early childhood, despite symptoms appearing between ages 6-12
Across global education and pediatric systems, ADHD frequently goes unrecognized despite symptoms commonly emerging in early childhood. While early recognition is critical for academic, emotional and social outcomes, delayed identification remains widespread. A key challenge is that early ADHD symptoms often overlap with typical childhood behaviours, making it difficult for caregivers to distinguish between normal development and clinically significant concerns.
It was a client project. I chose this project because it sits at the intersection of healthcare, education and behaviour-led design, where early intervention can significantly change outcomes. ADHD is often missed in its early stages due to limited awareness and lack of accessible screening tools. This project allowed me to explore how research-driven design can support early awareness and enable timely professional intervention.
Research-Driven Design Process
Understanding the brief
ADHD often goes unrecognized in early childhood due to symptom overlap with normal behavior. Although early identification improves academic, emotional and social outcomes, caregivers struggle to distinguish clinically significant patterns, revealing a need for clearer, supportive early-screening tools
Line of inquiry
- What factors contribute to ADHD going unrecognized in early childhood and who are the stakeholders and how do they perceive and interpret early symptoms that often resemble typical behaviours?
- Are there any social, awareness or systemic barriers which lead to ADHD going unnoticed or ignored.
- And how do varying perspectives influence who feels responsible for identifying potential signs and initiating early screening in the first place?
Literature Review
Behaviour appears developmentally typical
Early inattention, hyperactivity, and emotional variability resemble normal childhood behaviour, making impairment difficult to judge. (Wolraich et al., 2019)
Context-dependent reporting
Parents and teachers often report symptoms differently across settings, leading to hesitation and delayed screening. (De Los Reyes & Kazdin, 2005)
Less disruptive symptoms overlooked
Inattentive presentations are less likely to trigger concern because they cause fewer behavioural disruptions. (Willcutt et al., 2012)
Comorbidity obscures identification
Anxiety, mood, or learning difficulties may mask ADHD or be addressed first. (Cortese et al., 2022)
Systemic and social barriers
Stigma, limited awareness, insufficient screening time, and poor coordination between schools and healthcare delay identification. (Visser et al., 2015; Wolraich et al., 2019)
Clinical implication
ADHD frequently co-occurs with depression, reinforcing the need for early, routine screening that also considers emotional symptoms. (Cortese et al., 2022; Garcia-Argibay et al., 2024)
Stakeholder & Ecosystem Mapping
Parents / Primary Caregivers
Home context, daily observations
Class Teacher
Classroom behavior, academic tracking
Family Doctor
First medical point of contact
School Administrator
Policy, support systems
Developmental Pediatricians
Specialist assessment
Child Psychologists
Behavioral evaluation
Psychiatrists
Diagnosis & medication
Behavioral Therapists
Intervention strategies
Occupational Therapists
Sensory & motor support
Subject Teachers
Cross-subject observations
School Counselors
Emotional support
Special Educators
Resource teachers
Tuition / Coaching Centers
After-school learning context
Extended Family
Generational views on behavior
Peer Parents
Community comparison & support
Online Forums & WhatsApp Groups
Informal information exchange
Social Media & Misinformation
Cultural beliefs, stigma
Education Boards
Curriculum & inclusion policies
Insurance Systems
Coverage for assessments
School Inclusion Policies
Accommodation frameworks
Healthcare Policy Bodies
Standards & guidelines
Primary Care Clinics
First screening access point
Contextual Enquiry
Methods Used
Field Visits
- Classrooms: Attention demands, behavioral expectations, reporting mechanisms
- Homes: Parental interpretation, coping strategies, normalization or concern
- Primary care settings: Time-limited consultations, screening workflows, referral decisions
- School-clinic coordination: Information handoff and follow-up gaps
Stakeholder Interviews (Semi-Structured)
- 8 teachers
- 10 parents
- 2 psychologists
Surveys
- 35 parents
- 32 teachers
- 4 psychologists
Research Goals
Primary Research Insights
Parents
Sample size: 35Teachers
Sample size: 32Psychologists
Sample size: 4Research Gigamap
Journey Mapping, Personas & Affinity Mapping
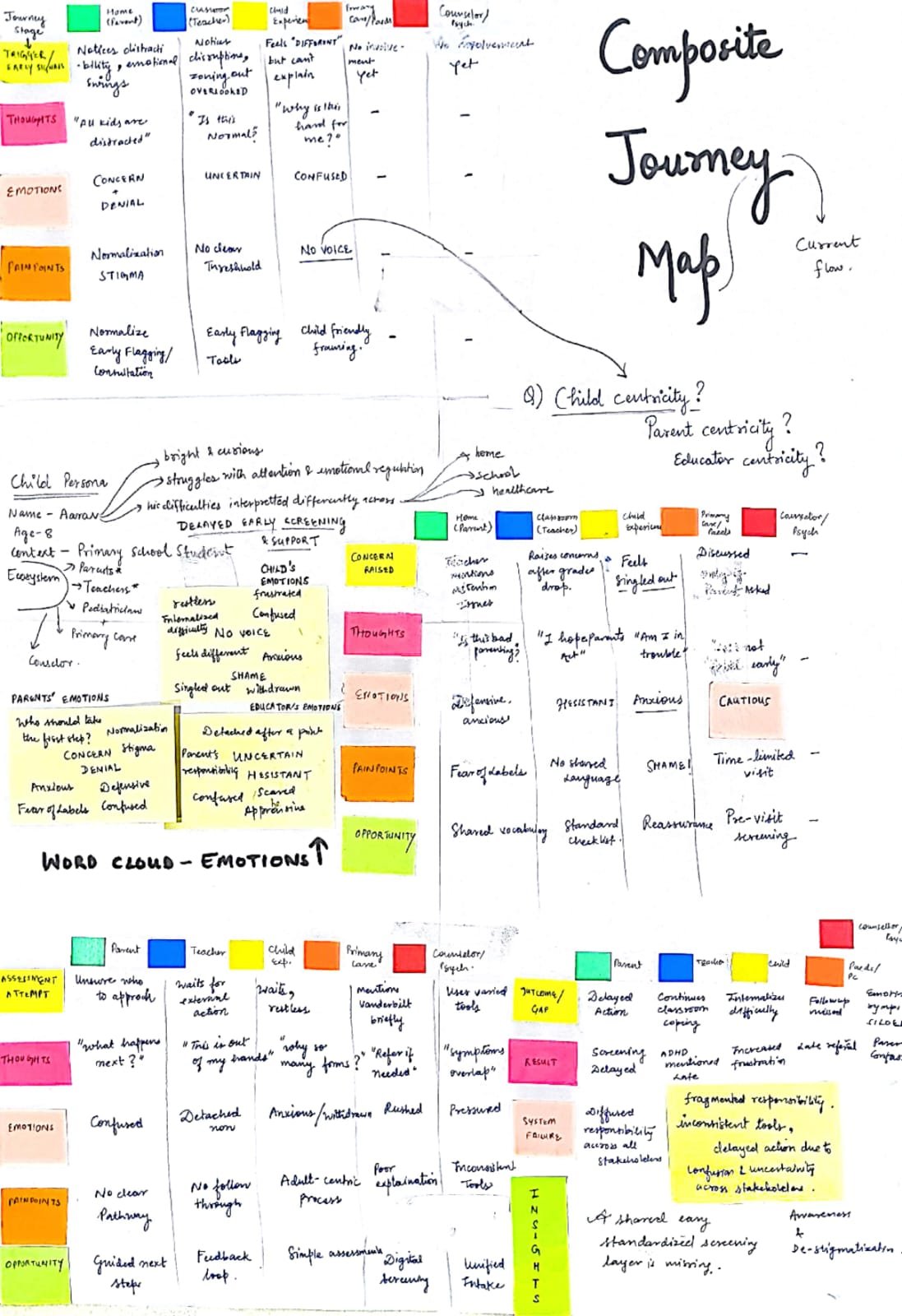
Primary & Secondary Research Insights
Iteration 1 — Identifying Themes for each Stakeholder Group
Clustering Themes
Awareness & Knowledge Gaps
Barriers & Stigma
ADHD & Depression are co-morbid
Communication Breakdowns
Practical Workflow Constraints
Suitability of Screening Tools
Synthesising & Ideation
ADHD is often missed early due to symptom overlap with normal childhood behavior and inconsistent interpretation across home and school contexts.
Contextual inquiry revealed fragmented observations, unclear ownership of screening, and lack of shared documentation between parents, teachers and clinicians.
Literature highlights frequent ADHD comorbidity with mood disorders, increasing the risk of missed or delayed identification.
Standardized, validated tools (Vanderbilt for ADHD and CES-DC for depressive symptoms) address variability and capture co-occurring risks.
Crazy 8
Classroom Observation Tool
Hits data capture + Doesn’t support diagnosis
Parent Support Companion + Data Capture + Expert Payoff Insights
Helps immediate classroom management + Low-tech & scalable
Awareness Workshops + Resources
Needs verified doctors + Higher institutional cost. Empathy + belonging + accelerates professional help
Gamified Screening Tool
Easy to validate clinically + requires long iterative research. Data-driven & engaging + standardized
CRAZY 8
8 rapid ideation concepts
Observe, Model & Activity Exercise Insights
Continuous tracking + Supports narrative over score-based approach. High scaffolding impact
Validated Screening Test for Children
Personalized insights + Data-driven screening & tracking. Requires more data first + objective vs screening
Wearable + Sensory Monitor
Hardware cost + Not useful without prior screening baseline. Continuous tracking + Supports objective data
ADHD Parent Community App
First step before clinical assessment. Dependent on self-reporting accuracy + May need cultural interpretation
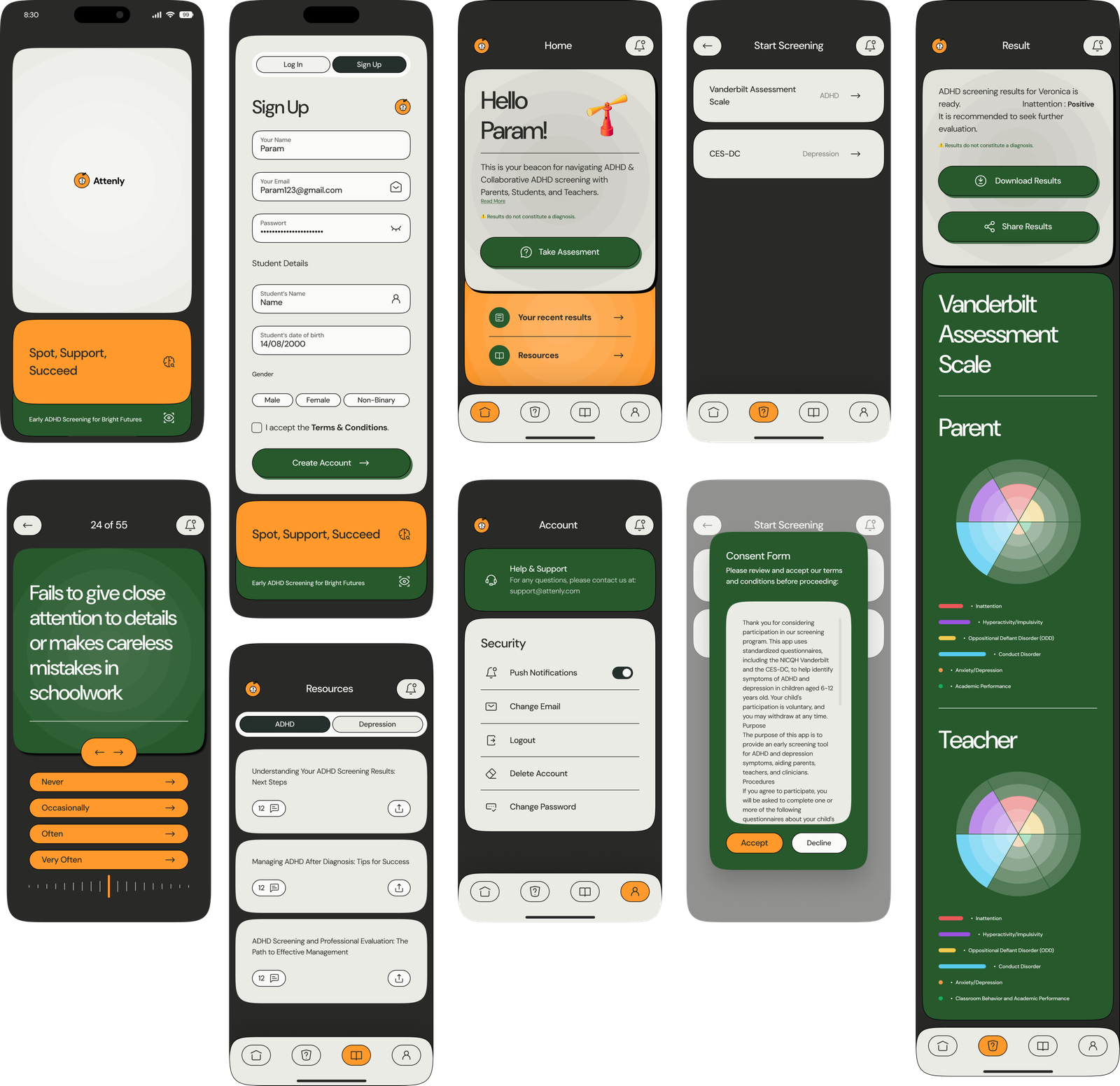
Envisioning Attenly - A Child Centric, Collaborative ADHD Screening app for parents and teachers
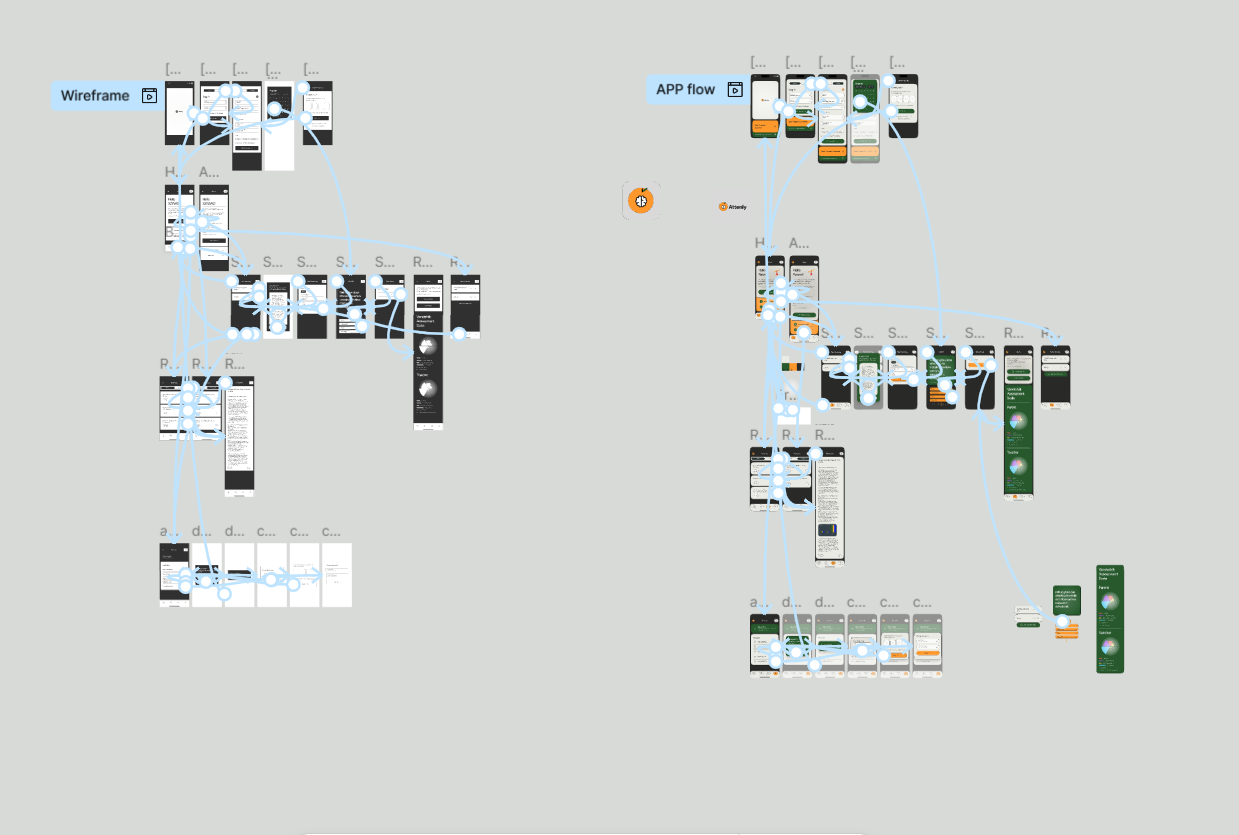
Information Architecture & Wireframes
Information Architecture
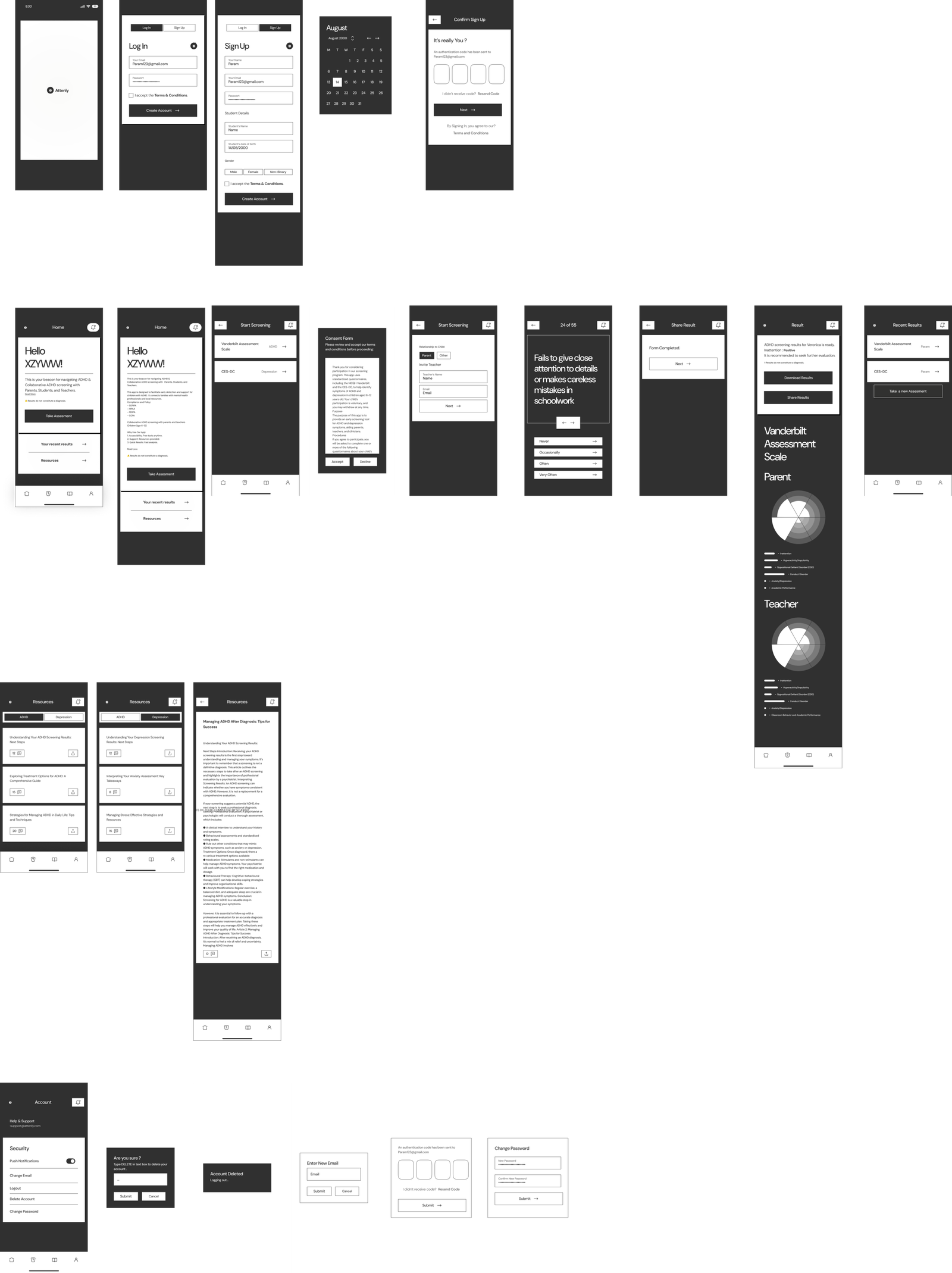
Low-Fidelity Wireframes
Composite User Journey
Post Attenly
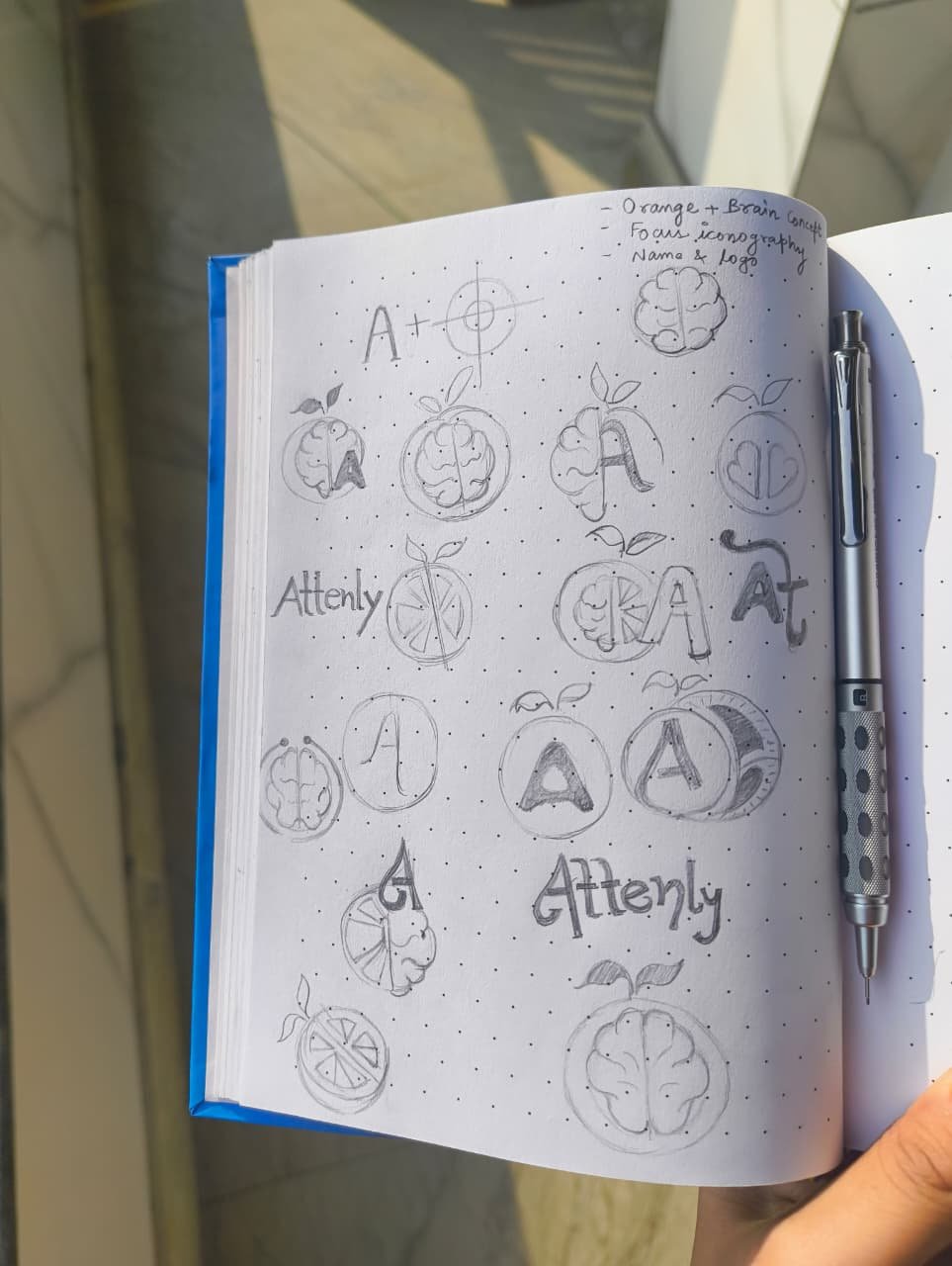
Brand Identity
Color Palette
Deep Forest Green
Warm Orange
Charcoal
Soft Cream
Few Screens at Glimpse
High Fidelity
Prototyping